XYMOGEN, K2-D3 Max 60 Capsules
K2-D3 Max is formulated for those who need a more substantial presence of vitamin K2, delivering 180 mcg per serving. The combination of highly bioavailable and bioactive menaquinone-7 (MK-7) with vitamin D3 provides complementary benefits for bone and cardiovascular health.*
- Supports Bone Health*
- Promotes Carboxylation of Bone Proteins*
- Supports Cardiovascular Health and Arterial Elasticity*
Vitamin K (as MK-7)
The body has limited vitamin K storage capacity compared with other lipophilic vitamins. Vitamin K rapidly depletes without regular dietary intake, yet a small reserve is recycled through a complex oxidation–reduction cycle. The primary function of vitamin K is as a cofactor in producing blood coagulation factors in the liver. Vitamin K also has rather complicated physiological roles in the carboxylation of the proteins involved in promoting bone mineralization and inhibiting arterial calcification.1,2 These physiological roles directly affect bone health and arterial elasticity, respectively.*2,3
Supplemental vitamin K can be found in the 3 following forms: synthetic K1; menaquinone-4 (MK-4), which is structurally similar to K1; and natural, long-chain menaquinone-7 (MK-7), which provides the highest vitamin K activity.4 Structural variations between K1 and K2 impact their bioavailability and bioactivity. Menaquinone-7, with its longer side chain, is very hydrophobic. Compared with K1, the physiochemical properties of MK-7 make it highly transportable by plasma lipoproteins, increase its extrahepatic (bones, arteries, etc) availability, and result in its long half-life.2,5,6 Findings from a series of studies comparing the in vivo properties of orally administered K1 and MK-7 demonstrated better bioavailability and utilization of MK-7.*2
Bone Health
Through carboxylation, vitamin K activates osteocalcin, the protein needed to bind calcium to the mineral matrix in bone. A 2020 review concluded that MK-7 has the highest bioavailability and the most significant effect on human osteocalcin carboxylation.7 Several studies have demonstrated the efficacy of MK-7 in increasing the carboxylated-to-uncarboxylated osteocalcin (cOC:ucOC) ratio. A high cOC:ucOC ratio is associated with bone health.2,5,6,8 Results from phase 1 of a dose-finding, randomized, double-blind, placebo-controlled trial (N = 60) support that 100 mcg of MK-7 is an effective minimum dose for improving osteocalcin carboxylation. When phase 2 (N = 120) used the placebo or 100-mcg MK-7 dose for 12 weeks with a controlled diet, the test group showed a significant increase in the cOC:ucOC ratio compared with the placebo, confirming the improvement of bone health indices.5 In a randomized, double-blind, placebo-controlled trial in healthy postmenopausal women (N = 244), the test group subjects received 180 mcg of MK-7 daily for 3 years. Supplementation of MK-7 significantly improved vitamin K status and a decrease was seen in measurements of age-related bone loss.*8
Arterial/Cardiovascular Support
Vitamin K participates in the carboxylation of matrix GLA protein (MGP), a protein regarded as the most potent inhibitor of arterial calcification, and the intake of long-chain MK is inversely correlated with calcium accumulation in arteries.4,6,9 Conversely, during vitamin K insufficiency, MGP is produced in its inactive form, which is associated with increased cardiovascular risk.10 Arterial calcification makes arteries stiff and less able to expand and contract. In a double-blind, placebo-controlled trial, 244 healthy postmenopausal women were given 180 mcg/d of MK-7 and followed for 3 years using pulse wave velocity and ultrasound techniques to determine changes in local carotid and regional aortic stiffness. At the conclusion of the study, the Stiffness Index ß in the MK-7 group had decreased significantly compared with a slight increase in the placebo group. Results confirmed that MK-7 inhibited age-related stiffening of the artery walls and significantly improved vascular elasticity.11 Reviews of the research results evaluating the relationship between vitamin K2 and cardiovascular health suggest a reduction in the mortality rate related to arterial calcification with vitamin K2 intake.*4,12
Vitamin D (as D3)
Vitamin D3 deficiency is common and widespread.13 Many factors can affect D3 biosynthesis, including time of day, seasons, location, smog/pollution, clothing, skin tone (darker skin requires more sun exposure), sunscreen use, low-cholesterol diets, and certain cholesterol therapies. The body needs vitamin D to absorb calcium, and the importance of vitamin D in skeletal health and bone density is well-established. Without adequate absorption, the body must take calcium from its skeletal stores, which weakens existing bone and prevents the formation of strong, new bone. Research results indicate that vitamin D deficiency coexists with low bone mineral density and vitamin D insufficiency is a common risk factor for osteoporosis associated with increased bone remodeling and low bone mass.14 A pooled analysis evaluating 11 randomized, double-blind, placebo-controlled trials concluded that vitamin D supplementation (>800 IU daily) was favorable in maintaining hip and nonvertebral bone integrity in individuals aged 65 and older.*15
There is also evidence for the role of vitamin D3 in arterial elasticity. In a double-blind, randomized controlled study, researchers sought to determine the differential effects of vitamin D3 supplementation in a group at high risk for cardiovascular disease. Subjects (N = 70) with serum 25-hydroxyvitamin D levels ≤20 ng/mL were randomized to oral supplementation of 600, 2,000, or 4,000 IU/d of vitamin D3 or placebo for 16 weeks. Vitamin D3 supplementation resulted in dose-dependent increases in serum 25-hydroxyvitamin D concentrations. Doses of 2,000 or 4,000 IU/d reduced arterial stiffness, as measured by carotid-femoral pulse wave velocity (cfPWV), with the decrease in cfPWV significantly greater in the 4,000-IU/d group (−10.4%) compared with the 2,000-IU/d group (−2.0%).*16
K2-D3 Max provides MK-7 and vitamin D3 at clinically studied levels to support bone and cardiovascular health in complementary ways.*
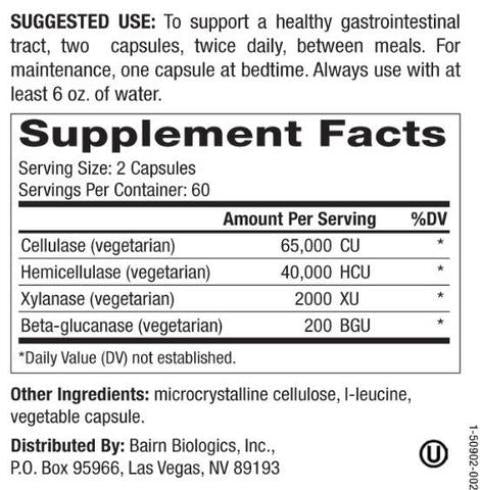
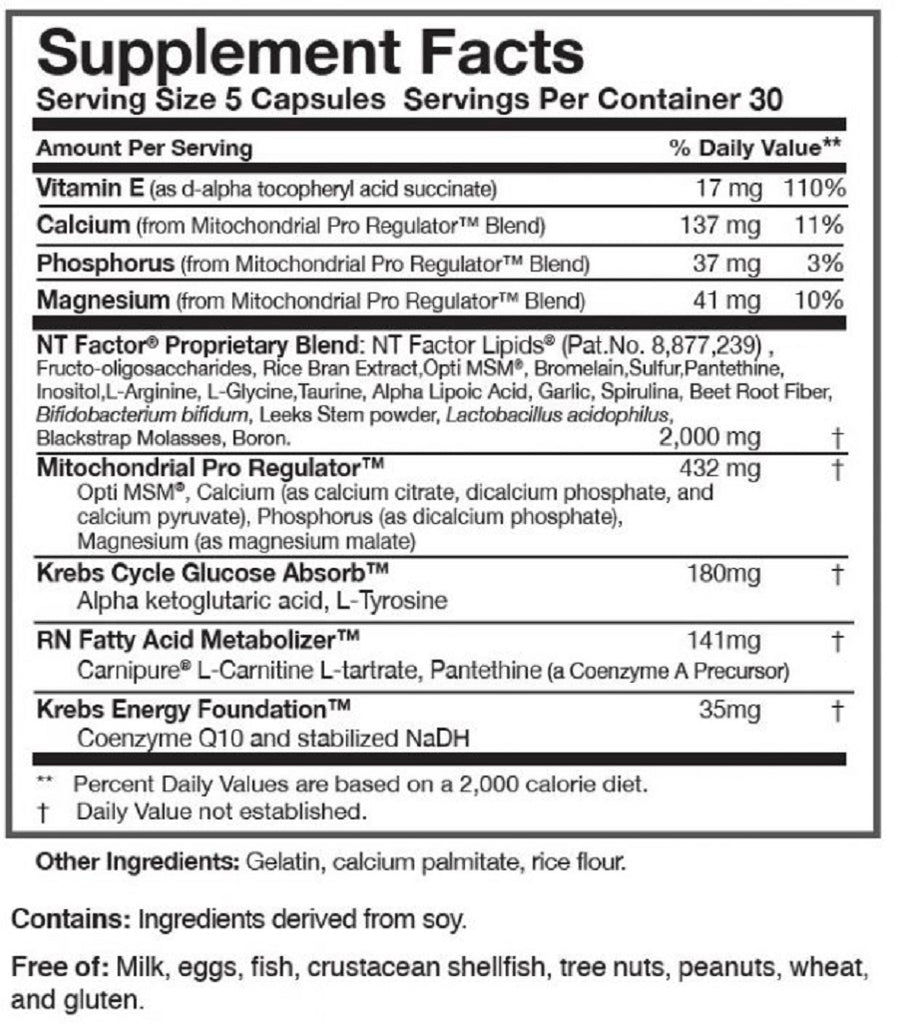
Other Ingredients:
Microcrystalline cellulose, capsule (hypromellose and water), ascorbyl palmitate, and silica.
Directions:
Take one capsule daily, or use it as directed by your healthcare professional.
Consult your healthcare professional before use. Individuals taking blood thinners or other medication should discuss potential interactions with their healthcare professional. Do not use it if the tamper seal is damaged.
Storage:
Keep closed in a cool, dry place out of reach of children.
Formulated To Exclude:
Wheat, gluten, yeast, soy protein, dairy products, fish, shellfish, peanuts, tree nuts, egg, sesame, ingredients derived from genetically modified organisms (GMOs), artificial colors, artificial sweeteners, and artificial preservatives.
References:
- Linus Pauling Institute. Vitamin K. Updated July 2014. Accessed October 4, 2022. https://lpi.oregonstate.edu/mic/vitamins/vitamin-K
- Schurgers LJ, Teunissen KJ, Hamulyák K, et al. Blood. 2007;109(8):3279-3283. doi:10.1182/blood-2006-08-040709
- Guo J, Fujiyoshi A, Willcox B, et al. Hypertension. 2017;69(1):102-108. doi:10.1161/HYPERTENSIONAHA.116.08459
- Maresz K. Integr Med (Encinitas). 2015;14(1):34-39.
- Inaba N, Sato T, Yamashita T. J Nutr Sci Vitaminol (Tokyo). 2015;61(6):471-480. doi:10.3177/jnsv.61.471
- Brugè F, Bacchetti T, Principi F, et al. Br J Nutr. 2011;106(7):1058-1062. doi:10.1017/ S0007114511001425
- Sato T, Inaba N, Yamashita T. Nutrients. 2020;12(4):965. doi:10.3390/nu12040965
- Knapen MH, Drummen NE, Smit E, et al. Osteoporosis Int. 2013;24(9):2499-2507. doi:10.1007/s00198-013-2325-6
- Theuwissen E, Cranenburg EC, Knapen MH, et al. Br J Nutr. 2012;108(9):1652-1657. doi:10.1017/S0007114511007185
- Vermeer C, Vik H. Vascul Dis Ther. 2020;5:1-4. doi:10.15761/VDT.1000179.
- Knapen MH, Braam LA, Drummen NE, et al. Thromb Haemost. 2015;113(5):1135- 1144. doi:10.1160/TH14-08-0675
- Flore R, Ponziani FR, Di Rienzo TA, et al. Eur Rev Med Pharmacol Sci. 2013;17(18):2433-2440.
- Taha R, Abureesh S, Alghamdi S, et al. Int J Gen Med. 2021;14:3849-3870. doi:10.2147/IJGM.S317421
- Laird E, Ward M, McSorley E, et al. Nutrients. 2010;2(7):693-724. doi:10.3390/nu2070693
- Bischoff-Ferrari HA, Willett WC, Orav EJ, et al. N Engl J Med. 2012;367(1):40-49. doi:10.1056/NEJMoa1109617
- Raed A, Bhagatwala J, Zhu H, et al. PLoS One. 2017;12(12):e0188424. doi:10.1371/journal.pone.0188424.